Discover what kratom detox is, how long kratom detox takes, and how ibogaine-assisted treatment can help.
Use of products made from the leaves of Mitragyna speciosa, commonly known as kratom, has quietly gained popularity in the United States.1
Even if the name “kratom” is unfamiliar, you’ve likely passed by advertisements for it on neon signs outside vape shops, at the checkout counter of your local gas station, or in online forums like Facebook Marketplace.
Novel Research on Ibogaine-Assisted Therapy for Kratom Withdrawal Symptoms
At Beond, we’ve witnessed the negative effects of kratom dependence firsthand. Recently, an increasing number of high-functioning people like Jane* have sought our help for their problematic kratom use, often after years of daily consumption and failed attempts to stop.
When researching best practices on how to help our clients with kratom dependence, we discovered they simply don’t exist; there are no clinical studies on ibogaine-assisted treatment for kratom withdrawal.
Driven by the desire to address this unmet need, we conducted a study on the impact of ibogaine treatment on kratom withdrawal symptoms.
In terms of detoxification, kratom’s withdrawal symptoms overlap significantly with those of typical opioids. Therefore, our clinical team felt that we could adapt our established ibogaine-assisted opioid detoxification protocols to the detoxification of kratom.
How Long Does Kratom Detox Take and What is Kratom Withdrawal Like?
Is kratom addictive? Like traditional opioids, kratom use can lead to dependence. Habitual users can experience profound impacts on quality of life while using the drug, as well as opioid-like withdrawal symptoms upon stopping.
Chronic kratom use can cause constipation, fatigue, insomnia, and emotional blunting. Jane described her experience of kratom withdrawal symptoms, saying:
“If you took too much [kratom], you get really tired and feel icky, like you’re gonna get sick.…Emotionally, I would say it knocked your feelings, so you don’t really have those real feelings anymore. Towards the end…, no matter how much you took, it really wouldn’t do anything.”
Withdrawal from kratom, while often milder than those associated with typical opioids, can still involve anxiety, insomnia, restlessness, depression, and physical pain. These uncomfortable withdrawal symptoms often motivate kratom users to return to the drug or “street opioids,” despite the obvious negative consequences.
Cold turkey kratom detox typically lasts 4-7 days, though the duration can vary depending on use.

What is Ibogaine?
Ibogaine is a psychoactive alkaloid extracted from the root bark of Tabernanthe iboga, a Central West African plant consumed ceremonially for centuries by the Bwiti people of Gabon and other African regions.
Ibogaine clinics predominantly utilize ibogaine derived from another African plant, Voacanga africana, as a more sustainable practice. Ibogaine interacts with multiple brain receptors relevant to addiction, mood regulation, and neuroplasticity. Of particular relevance to opioid and kratom use disorders, ibogaine contributes to its capacity to attenuate acute withdrawal symptoms of kratom by resetting neurochemical systems affected by opioid and kratom misuse.
Early clinical studies suggest that ibogaine can increase brain-derived neurotrophic factor expression to support synaptic plasticity.
This multifaceted combination of neurotrophic support positions ibogaine as a unique candidate for addressing the intertwined neurobiological substrates of substance use disorders and associated mood dysregulation.

Beond’s Ibogaine-Assisted Kratom Detox Protocol
To study whether our opioid detoxification program would be just as effective for kratom, we studied 24 guests who enrolled in our Chemical Dependency program for problematic kratom use.
We followed our guests through a 14-day medically supervised program that included the withdrawal management period, administration of an ibogaine flood dose, followed by one or more supplementary doses.
Guests with problematic kratom use were enrolled in a longer program duration (14 vs. 10 days) due to the extended time it takes for kratom to be eliminated from the body and its complex pharmacological dynamics that sometimes require additional time in recovery.
Prior to ibogaine treatment, participants received electrolyte supplementation and underwent kratom detoxification under our opioid withdrawal management protocol.

Withdrawal symptom severity was measured using two standardized scales administered at 24-hour intervals: the Subjective Opiate Withdrawal Scale (SOWS) and the Objective Opiate Withdrawal Scale (OOWS), from baseline through 120 hours post-ibogaine treatment.15
Through the administration of these two scales which quantify both the subjective symptoms reported by the patient, such as body aches, and the number of objective symptoms of detoxification reported by a clinical staff member, such as restlessness and hand tremors, Beond’s clinician-researchers received a complete before and after picture of the withdrawal experience of each participant.
Results: Ibogaine Treatment Decreases Kratom Withdrawal Symptoms
Gratifyingly, study participants showed significant reductions in withdrawal symptoms following ibogaine administration. Subjective reports of withdrawal symptoms dropped significantly from pre-treatment levels by 50% at the first time point (24 hours post-ibogaine treatment) and continued to decrease to 74% at the final time point (120 hours post-ibogaine treatment).
A similar impact was observed on the number of objective withdrawal symptoms (out of 13); OOWS scores dropped significantly by 61% in 24 hours and remained low through all timepoints measured, with an average reduction of 78% at the final time point.
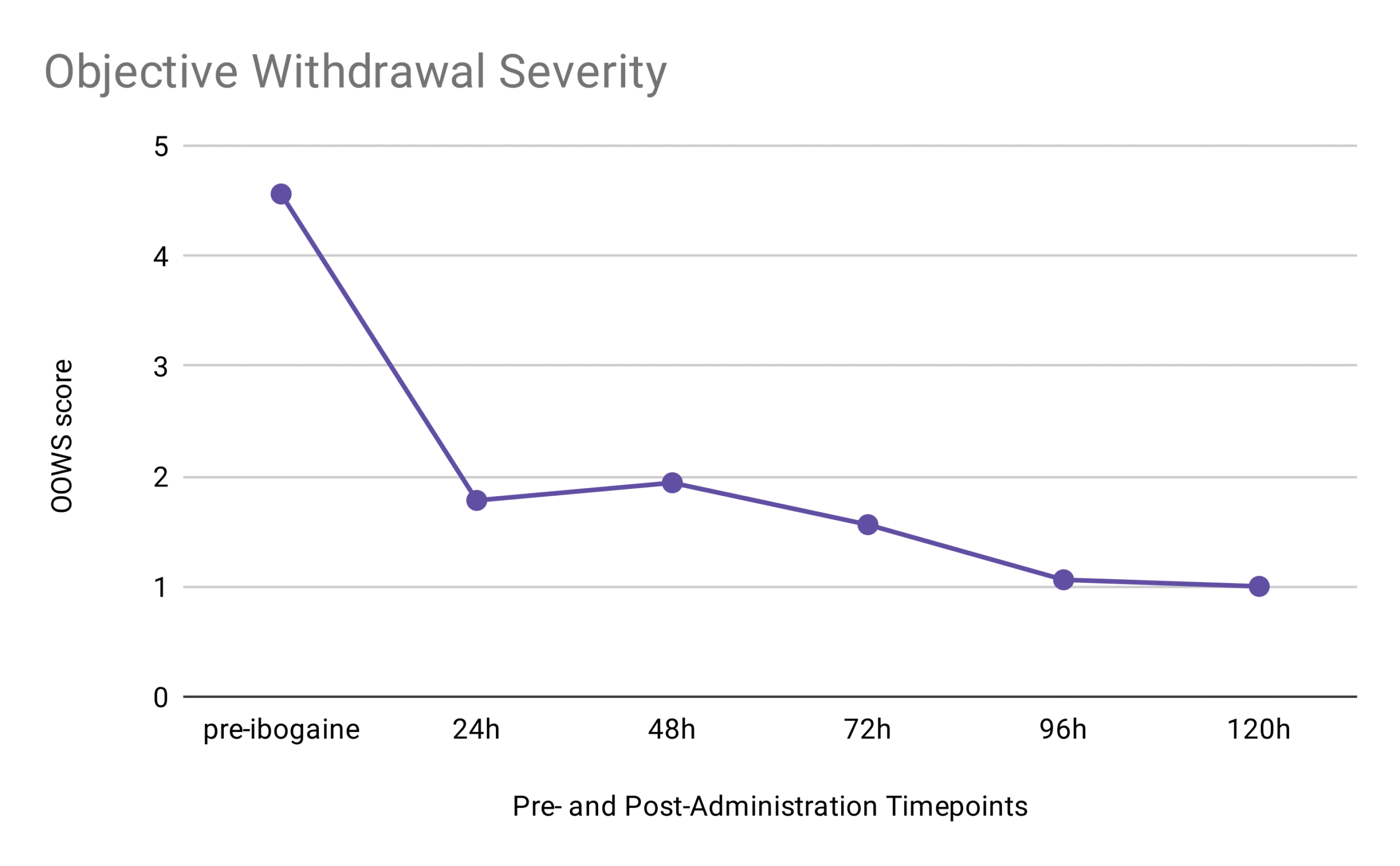
OOWS Caption: The study participants experienced a 78% reduction in objective withdrawal symptoms between pre-treatment and 120 hours post-treatment.
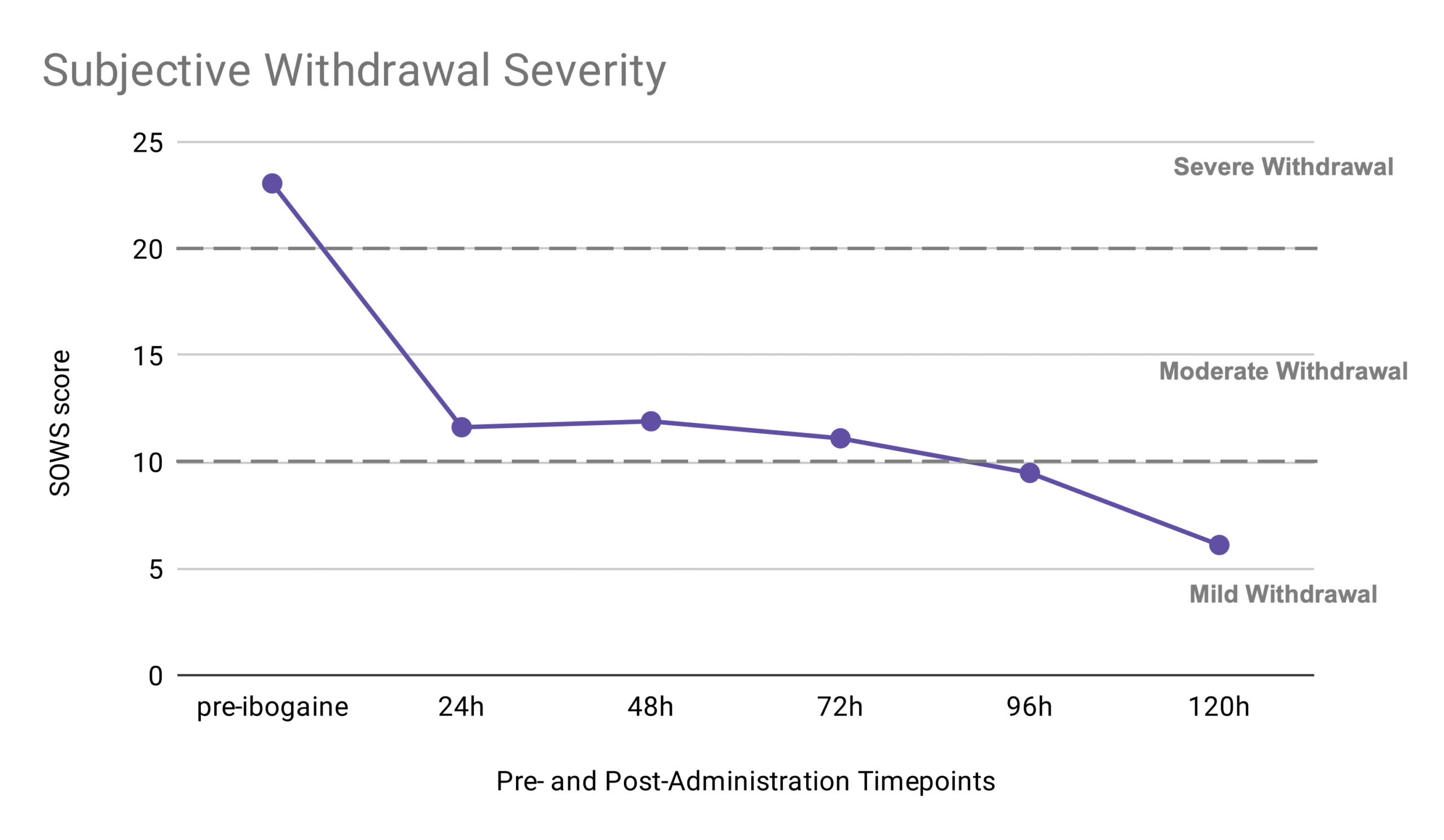
SOWS Caption: The study participants experienced a 74% reduction in subjective withdrawal scores between pre-treatment and 120 hours post-treatment.
These results suggest ibogaine-assisted therapy protocols for typical opioids can be readily adapted to kratom detox.
Additionally, the new kratom detoxification protocol seems to provide a significant improvement over the conventional, cold-turkey approach. Kratom users who quit the drug without transferring to an opiate replacement and/or ibogaine treatment can expect a 4-7-day withdrawal period marked by physical and psychological distress.
In contrast, study participants experienced a notable decrease in both the intensity and duration of these withdrawal symptoms. Considering that the painful experience of withdrawal symptoms is a major risk factor for relapse, the lessening of such symptoms is likely to improve recovery outcomes.
Kratom’s Neurochemical Impact on Pain and Addiction
While some kratom users report taking the drug for a euphoric, opioid-like high, many others use it to self-manage conditions such as pain, fatigue, and anxiety.2-6
The natural chemicals in kratom interact with multiple brain systems, often producing effects that users report as beneficial.7
Jane described her early experiences with the drug:
“I was just kinda dealing with situational depression, lack of energy, and motivation. I would take, like, four or five pills and [it would] give me energy and motivation. It just kept me away from alcohol… nobody would tell that I was on it.”
The effect of its natural chemical compounds on the opioid receptors also makes kratom an increasingly popular self-treatment for opioid withdrawal symptoms or chronic pain, keeping consumers from purchasing unsafe, non-pharmaceutical “street” opioids.8 When ingested, kratom’s primary active compound, mitragynine, partially activates the mu opioid receptor, which is the same receptor targeted by opioids like heroin and fentanyl. This molecular interaction is key to kratom’s appeal as both a substitute for opioids in dependent individuals and an over-the-counter analgesic.
The chemical compounds found in kratom have demonstrated pain-reducing properties in both animal models of pain and self-reported human studies. In a survey of 2,798 kratom users primarily residing in the US, 91% reported using the drug as a long-term substitute for opioids like OxyContin or other pain-relievers. Pain management was also one of the most commonly reported motivations for kratom use by these individuals.9
Despite these preliminary laboratory and survey results, however, human studies regarding kratom’s pain-relieving properties are lacking.
Kratom: A Safer Alternative to Opioids?
Uniquely, mitragynine activates the mu opioid receptor only partially and without engaging the β-arrestin pathway responsible for many negative side effects, including respiratory depression. In short, mitragynine has a minimal risk of the life-threatening adverse effects seen in opioid overdose, contributing to kratom’s popularity as what some would consider a “safer alternative” to typical opioids.10
Additionally, the time it takes for mitragynine to be eliminated from the human body is substantially longer than that of typical shorter-acting opioids, taking up to two days or longer, depending on volume of use.11
In this respect, mitragynine can be comparable to the longer acting opiate, methadone, one of the mainstay treatments for opioid dependence.
Considering mitragynine’s apparent benefits, it’s not hard to see why kratom has sparked interest as a potential new pharmacotherapy for pain and/or addiction. As a result, several kratom advocacy groups, including the American Kratom Association and Protect Kratom, are fighting to protect access to what they claim is a safe and beneficial botanical supplement.
While mitragynine has an improved safety profile when compared to typical opioids, it’s far from benign. In fact, mitragynine’s metabolites, 7-hydroxymitragynine (also called 7-OH) and mitragynine pseudoindoxyl, are actually more potent at the mu opioid receptor than morphine (by roughly 10 times and 40 times, respectively).12,13
It is currently unclear whether these metabolites are capable of producing life-threatening respiratory depression or not.
Further research into the safety of these compounds is needed, especially considering the emergence of concentrated 7-OH and mitragynine pseudoindoxyl products within the past year.14
Despite the opioid-like properties of mitragynine and its metabolites, kratom remains federally unregulated and legal in most states. This seems likely to change, however.
In July 2025, the FDA took the first steps towards scheduling 7-OH, citing the health concerns resulting from its potent mu opioid receptor activity.
The Challenge and Promise of Ibogaine Treatment for Kratom Addiction
While the results of our study are promising, ibogaine shouldn’t be considered a silver bullet. Ibogaine treatment requires active participation and integration to have a positive and lasting effect. Therefore, it isn’t a good fit for individuals looking for a quick fix.
For many, ibogaine induces an intense, visionary state often described as emotionally and spiritually charged. In the safe and supportive environments provided at Beond, this may help individuals uncover the root cause of their substance misuse. For Jane, the experience was both disorienting and deeply clarifying:
“[The ibogaine experience was an] absolute crazy mess. But, at this point it makes sense and I know it will continue to make perfect sense. Organized chaos. [A] roller coaster ride of sadness, fear, grief, and loneliness. When I returned to the recovery room, I started putting things together and everything started making sense.”
Jane’s testimony highlights the work required to successfully integrate the often-intense ibogaine experience.
Is Ibogaine Safe for Kratom Detox?
Ibogaine also carries the potential of medical risks, particularly cardiac complications like QTc prolongation that may lead to arrhythmia, a change in the rhythm of the heart.
It is common for those receiving ibogaine treatment to exhibit QTc prolongation, but with our rigorous and continuous cardiac monitoring safety methodologies during ibogaine treatment, our guests in the study sample did not experience any emergency adverse events.
The necessity for continuous cardiac monitoring underscores why ibogaine should only be administered by experienced clinicians in specialized, medically-equipped settings.
Despite its challenges, many patients describe ibogaine-assisted therapy as not just a detox but as an emotional and spiritual reset, offering perspective on life events and patterns of behavior that contributed to substance use. At her one-month follow-up, Jane reported no kratom use — an outcome resulting from her increased insight and commitment to the ongoing work of addiction recovery:
“[My kratom use after ibogaine has been] zero. I threw everything away before I left. I have to maintain that… If I’m not doing the correct things, all it takes is a bad day. The motivation, yeah, it’s still coming. It’s there … it would get better, but it just takes a little longer than that.”
The Current and Future Impact of the Study Results
In this blog post, we’ve provided a sneak peek at our unpublished data supporting the effectiveness of ibogaine-assisted therapy in lessening kratom withdrawal symptoms.
We hope that by openly sharing these results, we will expedite the safe and effective application of ibogaine-assisted therapy to the growing and underserved population of individuals who experience kratom misuse or dependency.
Given the growing number of people with kratom dependence and the lack of evidence-based treatments, the development of protocols for kratom detox is both acutely relevant and highly innovative.
Ibogaine-assisted therapy is particularly impactful, as it treats kratom dependence without relying on long-term opioid substitution regimens (e.g., buprenophine, methadone). This is hugely meaningful for individuals who have developed a dependence on kratom after using it as a replacement for typical opioids.
The data shared here are only the beginning. Our future work will track long-term outcomes such as cravings, abstinence rates, and quality of life for months and years after treatment. But for now, the message is clear: kratom dependence is real, it can be treated, and ibogaine-assisted detox may be one of the most effective tools we have.
If you or someone you love is interested in learning more about how ibogaine treatment may alleviate the symptoms of kratom withdrawal, please visit www.beondibogaine.com. Follow the prompts to sign up for Beond’s newsletter and schedule an informational consultation.
*Name changed to protect the identity of our previous guest.
References
Brown PN, Lund JA, Murch SJ. A botanical, phytochemical and ethnomedicinal review of the genus Mitragyna korth: Implications for products sold as kratom. Journal of Ethnopharmacology. 2017 Apr;202:302–25.
Suwanlert S. A study of kratom eaters in Thailand. Bulletin on narcotics. 1975;27(3):21–7.
Vicknasingam B, Narayanan S, Beng GT, Mansor SM. The informal use of ketum (Mitragyna speciosa) for opioid withdrawal in the northern states of peninsular Malaysia and implications for drug substitution therapy. International Journal of Drug Policy. 2010 Jul;21(4):283–8.
E. Adkins J, W. Boyer E, R. McCurdy C. Mitragyna speciosa, A Psychoactive Tree from Southeast Asia with Opioid Activity. Current Topics in Medicinal Chemistry. 2011 May 1;11(9):1165–75.
Stolt AC, Schröder H, Neurath H, Grecksch G, Höllt V, Meyer MR, et al. Behavioral and neurochemical characterization of kratom (Mitragyna speciosa) extract. Psychopharmacology. 2014 Jan 12;231(1):13–25.
Brown PN, Lund JA, Murch SJ. A botanical, phytochemical and ethnomedicinal review of the genus Mitragyna korth: Implications for products sold as kratom. Journal of Ethnopharmacology. 2017 Apr;202:302–25.
Eastlack SC, Cornett EM, Kaye AD. Kratom—Pharmacology, Clinical Implications, and Outlook: A Comprehensive Review. Pain and Therapy. 2020 Jun 28;9(1):55–69.
Boyer EW, Babu KM, Macalino GE, Compton W. Self‐Treatment of Opioid Withdrawal with a Dietary Supplement, Kratom. The American Journal on Addictions. 2007 Sep 10;16(5):352–6.
Mun CJ, Panlilio LV, Dunn KE, Thrul J, McCurdy CR, Epstein DH, Smith KE. Kratom (Mitragyna speciosa) use for self-management of pain: Insights from cross-sectional and ecological momentary assessment data. J Pain. 2025 Jan;26:104726.
Kruegel AC, Gassaway MM, Kapoor A, Váradi A, Majumdar S, Filizola M, et al. Synthetic and Receptor Signaling Explorations of the Mitragyna Alkaloids: Mitragynine as an Atypical Molecular Framework for Opioid Receptor Modulators. Journal of the American Chemical Society. 2016 Jun 1;138(21):6754–64.
Trakulsrichai S, Sathirakul K, Auparakkitanon S, et al. Pharmacokinetics of mitragynine in man. Drug Des Devel Ther. 2015;9:2421-2429.
Behnood-Rod A, Chellian R, Wilson R, Hiranita T, Sharma A, Leon F, et al. Evaluation of the rewarding effects of mitragynine and 7‐hydroxymitragynine in an intracranial self-stimulation procedure in male and female rats. Drug and Alcohol Dependence. 2020 Oct;215:108235.
Váradi A, Marrone GF, Palmer TC, Narayan A, Szabó MR, le Rouzic V, et al. Mitragynine/Corynantheidine Pseudoindoxyls As Opioid Analgesics with Mu Agonism and Delta Antagonism, Which Do Not Recruit β-Arrestin-2. Journal of Medicinal Chemistry. 2016 Sep 22;59(18):8381–97.
Hill K, Boyer EW, Grundmann O, Smith KE. De facto opioids: Characterization of novel 7-hydroxymitragynine and mitragynine pseudoindoxyl product marketing. Drug and Alcohol Dependence. 2025 Jul 1;272:112701.
Handelsman L, Cochrane KJ, Aronson MJ, Ness R, Rubinstein KJ, Kanof PD. Two New Rating Scales for Opiate Withdrawal. The American Journal of Drug and Alcohol Abuse. 1987;13(3):293-308.
Cover photo: Joe Raedle/Getty Images


